MicroRNA-gene signaling pathways in pancreatic cancer
p. 200
Alexandra Drakaki, Dimitrios Iliopoulos DOI:10.4103/2319-4170.119690 PMID:24225187
Pancreatic cancer is the fourth most frequent cause of cancer-related deaths and is characterized by early metastasis and pronounced resistance to chemotherapy and radiation therapy. Despite extensive esearch efforts, there is not any substantial progress regarding the identification of novel drugs against pancreatic cancer. Although the introduction of the chemotherapeutic agent gemcitabine improved clinical response, the prognosis of these patients remained extremely poor with a 5-year survival rate of 3-5%. Thus, the identification of the novel molecular pathways involved in pancreatic oncogenesis and the development of new and potent therapeutic options are highly desirable. Here, we describe how microRNAs control signaling pathways that are frequently deregulated during pancreatic oncogenesis. In addition, we provide evidence that microRNAs could be potentially used as novel pancreatic cancer therapeutics through reversal of chemotherapy and radiotherapy resistance or regulation of essential molecular pathways. Further studies should integrate the deregulated genes and microRNAs into molecular networks in order to identify the central regulators of pancreatic oncogenesis. Targeting these central regulators could lead to the development of novel targeted therapeutic approaches for pancreatic cancer patients.
Chronic allograft dysfunction: A model disorder of innate immunity
p. 209
Walter Gottlieb Land DOI:10.4103/2319-4170.117622 PMID:24225188
The innate immune system is a highly sensitive organ of perception sensing any cell stress and tissue injury. Its major type of response to all potential inciting and dangerous challenges is inflammation and tissue repair and, if needed, induction of a supportive adaptive immune response, the aim always being to maintain homeostasis. However, although initially beneficial, innate immunity-mediated, protection-intended repair processes become pathogenic when they are exaggerated and uncontrolled, resulting in permanent fibrosis which replaces atrophic or dying tissue and may lead to organ dysfunction or even failure. In this sense, atherosclerosis and organ fibrosis reflect classical disorders caused by an overreacting innate immune system. Strikingly, these two pathologies dominate the development of chronic allograft dysfunction as the main clinical problem still left in transplantation medicine. Growing evidence suggests that acute and chronic allograft injuries, including alloimmune-, isoimmune-, nonimmune-, and infection-mediated insults, not only lead to cell death-associated graft atrophy but also activate the innate immune system which, over time, leads to uncontrolled intragraft fibrogenesis, thereby compromising allograft function. Acute and chronic allograft injuries lead to induction of damage-associated molecular patterns (DAMPs) which, after recognition by pattern recognition receptors, activate cells of the innate immune system such as donor-derived intragraft fibroblasts and vascular cells as well as recipient-derived graft-invading macrophages and leukocytes. It is mainly the orchestrated action and function of these cells that slowly but steadily metamorphose the originally life-saving allograft into a poorly functioning organ of marginal viability.
Cisplatin, tegafur-uracil and leucovorin plus mitomycin C: an acceptably effective and toxic regimen for patients with recurrent or metastatic nasopharyngeal carcinoma
Background: This prospective phase II clinical trial evaluated the efficacy and toxicity of cisplatin, oral tegafur-uracil, leucovorin, and mitomycin C in patients with recurrent or metastatic nasopharyngeal carcinoma.
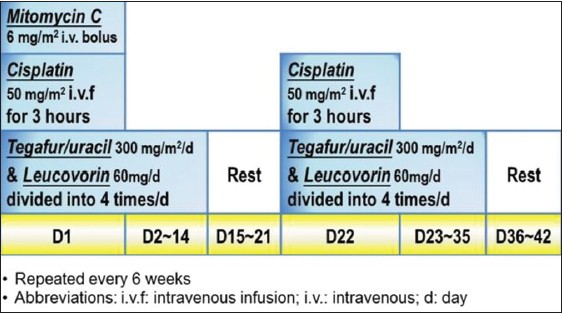
Methods: Patients with histologically proven non-keratinizing or undifferentiated nasopharyngeal carcinoma were prospectively enrolled from April 2002 to June 2005. Cisplatin 50 mg/m 2 on day 1, 22 and mitomycin C 6 mg/m 2 on day 1 were administered. Oral tegafur-uracil 300 mg/m 2 /day and oral leucovorin 60 mg/day were given on day 1-14 and day 22-35, respectively. Each cycle was repeated every 6 weeks. Primary and secondary endpoints are response rate and toxic profiles with survivals, respectively.
Results: Twenty-two patients with the median age of 47 (35-69) years were enrolled in the study. Sixteen (72.7%) patients had undifferentiated nasopharyngeal carcinoma. The regimen was well-tolerated by all patients with the exception of one patient (4.6%) who experienced grade IV anorexia, and two patients (9.1%) who had grade IV vomiting. There was no treatment-related death. The overall response rate was 59.1%, including 3 (13.6%) complete remissions. The median duration of response was 15.9 months, the median time to tumor progression was 10.0 months, and the median overall survival was 16.0 months.
Conclusion: This outpatient chemotherapy regimen is acceptably effective and toxic among patients with recurrent or metastatic nasopharyngeal carcinoma.
Background: Real-time ultrasound-guided techniques allow for improved cannulation of the internal jugular vein and femoral vein for hemodialysis; however, these techniques require extra sterilization procedures, specialized probes, or needle guides. A simpler ultrasound vessel localization method was performed to investigate whether this alternative approach would aid in the cannulation of the femoral vein for patients in whom temporary angioaccess was required for hemodialysis.
Methods: Patients requiring temporary femoral vein catheters for hemodialysis were divided into 2 groups on alternating days of the week during a 6-month period. One group underwent ultrasound localization of the femoral vein before cannulation and the second group received conventional landmark localization. Data regarding the strength of the femoral arterial pulse, number of attempts, failures, and complications were recorded.
Results: Ultrasound localization resulted in significantly improved first-attempt success rates, reduced attempts, and reduced failure and complication rates overall (p < 0.001, p < 0.001, p = 0.002 and p = 0.004 respectively) as well as in the group of patients with a clearly discernible arterial pulse (p < 0.001, p = 0.001, p = 0.004 and p = 0.011 respectively). The same trend was observed among patients with faintly palpable or non-palpable femoral arterial pulses, although the differences were not statistically significant.
Conclusion: Cannulation of the femoral vein for hemodialysis should be performed with the aid of ultrasound. If real-time ultrasound-guided cannulation is not available, the vessel localization method is a good alternative, given its known limitations and the fact that it is simpler. It remains to be determined whether 1 - dimensional localization or localization including vessel depth information can improve outcomes in patients with faintly palpable or non-palpable femoral arterial pulses.
Background: Health related quality of life (HRQOL) is an important issue for long-term kidney transplantation (KT) patients. Nevertheless, few studies have focused on long-term HRQOL in KT recipients with a functional graft. Thus, the aim of this study is to describe the long-term (10-year) HRQOL of KT recipients.
Methods: This is a cross-sectional and correlational design. The Medical Outcome Survey (MOS SF-36) questionnaire was used to collect data on HRQOL. The data were collected from November 2009 to September 2010 at a medical center in Northern Taiwan.
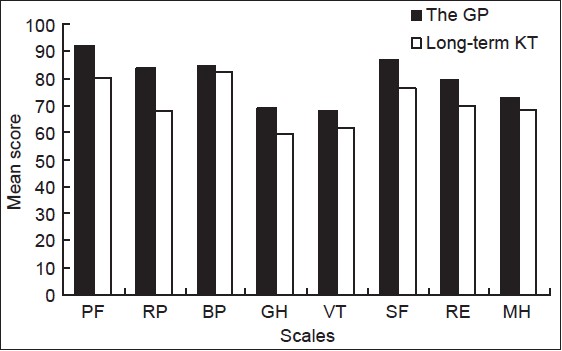
Results: A total of 88 patients were interviewed. The mean years after transplantation was 14.48 (SD = 3.9). The mean score of each of the HRQOL subscales ranged from 59.4 to 82.5. The mean scores on the bodily pain (BP) subscale were the highest and, on the general health (GH) subscale, the lowest. Compared to the general population, with the exception of the BP subscale, long-term KT patients had a lower mean score (poorer HRQOL) on all subscales. Age, gender, serum creatinine level, and employment status were significantly related to HRQOL.
Conclusion: HRQOL of long-term KT patients was, overall, poorer than that of the general population. When comparing the HRQOL of KT patients with that of the general population, one should take into account age and gender. Finally, the physical, psychological, and social adjustment domains of HRQOL of KT patients warrant further attention.
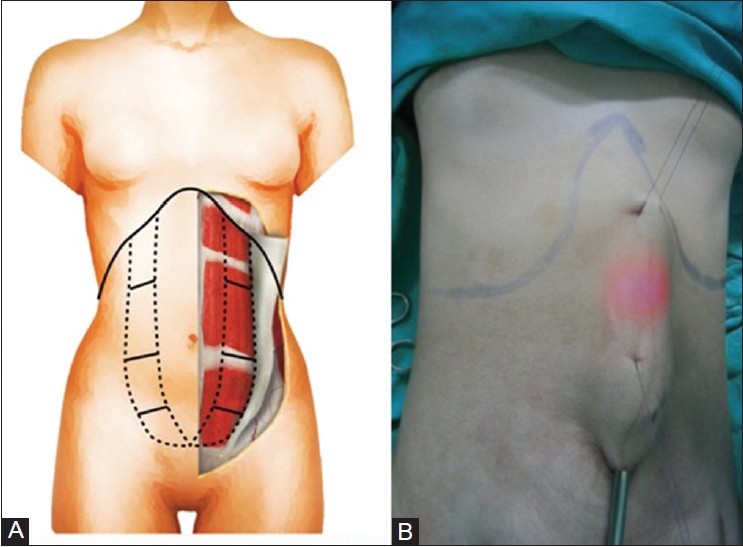
Background : The objective of this retrospective analysis was to assess the treatment of endoscope abdominoplasty for diastasis recti deformity patients.
Methods : From January 1999 to January 2011, 88 patients ranging from 35 to 46 years in age were treated with videoendoscopy-assisted minimally invasive surgery. All patients were Asian. Early (< 3 months) and late (> 6 months) complications were assessed throughout a follow-up period of up to 66 months.
Results : Observations were conducted at the end of three weeks, six months, and 66 months. Early on, all patients experienced numbness with local paresthesia (100%) closely after treatment, and reported the feelings to subside by six months post-treatment. Four patients (4.5%) experienced ecchymosis, and three patients (3.4%) were affected by seroma. One patient (1.1%) had dyspnea immediately after surgery, which recovered after oxygen (O 2 ) administration. Only one patient (1.1%) experienced minimal skin loss, which recovered after 3 months of surgery, and there were no further complications. Hypertrophic scars were apparent in three patients (3.4%) who showed no unwanted signs or further complications after post-operative scar care. No hematoma had been reported. All complications subsided (> 6 months) postoperatively.
Conclusions : Videoendoscopy-assisted abdominoplasty can be used for diastasis recti deformity with minimal excess skin. Our study demonstrated effects against the formation of seroma and other complications.